
Medical Associate Compensation Model
Choosing a Compensation Model
There are several compensation models for medical associates, each with its advantages and disadvantages. The most common models include:
- Salary: This is the most straightforward model, where the medical associate receives a fixed amount of money each year, regardless of the number of patients they see or the amount of work they do.
- Salary plus bonus: This model combines a base salary with a bonus based on performance, such as the number of patients seen or the amount of revenue generated.
- Commission: This model pays the medical associate a percentage of the revenue they generate. This model can be risky for the medical associate, as they may not earn any money if they do not see enough patients.
- Hourly rate: This model is based on the number of hours worked, and is typically used for part-time or temporary positions.
- Value-based compensation: This model rewards the medical associate for providing high-quality care, regardless of the number of patients they see or the amount of revenue they generate. This model is becoming increasingly popular as the healthcare industry moves towards value-based care but it is challenging to forecast since value can be subjective.
The best compensation model for a medical associate will vary depending on the individual’s needs and preferences. Some medical associates prefer the security of a fixed salary, while others are willing to take on more risk in exchange for the potential for higher earnings. Ultimately, the decision of which compensation model to use should be made after careful consideration of all the factors involved.
A Commission with Draw Approach
A Salary model, while straightforward, places most of the risk on the practice to fill the associate’s schedule. There is no incentive for the associate to market themselves or network to build their schedule. It also has the potential for the practice to overbook the associate to maximize profits.
A Salary plus bonus model addresses some of the concerns and risks mentioned above but presents new challenges in determining the base salary, bonus amount, and when it kicks in. It is typically structured as a base salary with a bonus when production exceeds a certain level. How do you determine the base salary relative to the bonus level? What is the bonus amount? It is difficult to predict how this will play out over time because there are many unknowns as well as salary and bonus amounts based on averages. The goal would be to find a sweet spot to have a stable income but also the opportunity to reach an achievable bonus threshold. The problem is that the sweet spot changes with time as the associate’s schedule builds.
A Commission model ties the compensation to the associate’s production but does not address the lack of initial income for an associate as they build their schedule. This is likely undesirable since the associate will be potentially coming out of school with living and school loan expenses and no income security.
A Commission with Draw approach can be structured as a Commission model with a Salary Draw. This means the associate’s compensation is based on a percentage of their generated revenue but they are provided a steady salary draw while they build their production. The compensation is periodically reconciled to determine if an additional amount is owed. Once the calculated compensation consistently exceeds the salary draw, then the salary draw can be increased to avoid a large difference accumulating. A Commision with Draw model is fundamentally a Commission model but provides the stability of a Salary model with a Salary plus bonus model built in – the best of all worlds and fair for both the practice and associate.
Cost to Practice
The practice can still maintain some flexibility in a Commission with Draw approach to reduce the risk of taking on an associate without knowing how long it will take for their production to cover their expenses. The salary draw can be increased as they are credentialed with additional insurance companies since they would initially have limited potential. The total cost and cost over time can be calculated by simulating some assumptions not only to give the practice an understanding of best and worst-case scenarios but also to help communicate to a potential associate what a compensation profile (or compensation over time) would look like.
Total Cost to Practice would include any benefits (e.g. health insurance, malpractice insurance), continuing education credits, licenses and dues, additional support staff, increased marketing costs, etc. These are included in the simulation as non-compensation expenses since they can vary significantly for any given offer and can be averaged as additional monthly expenses.
Medical Associate Compensation Simulation
A simulation provides the ability to run various scenarios helping to answer questions and address concerns before making a decision – data-driven decision!
Questions answered by a Medical Associate Compensation Simulation:
- How many patients does the associate need to see to cover their expenses?
- When will the associate’s production cover their expenses?
- What is the cumulative cost the practice needs to cover until the associate’s production covers their expenses?
- When does an associate’s total compensation exceed their cumulative salary draw?
Variables and Assumptions
Non-Compensation Associate Expenses (per month) – these include recurring monthly expenses that are not associated with compensation (e.g. malpractice insurance, license/CME/dues, health insurance (if offered), increase in marketing, additional support staff, etc.)
Compensation Expenses (per month) – for a Commission with Draw model, this would include a salary draw and commission rate. For a commission-only model, simply zero out the salary draw.
Revenue Variables – include the average charge per patient visit and the average reimbursement rate. It makes sense to choose conservative values here to reduce some risk.
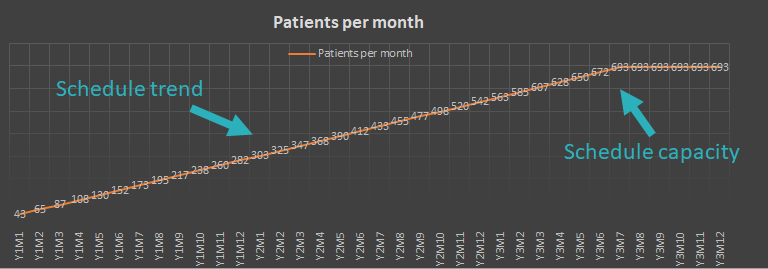
Production Profile (Capacity) – this helps calculate the maximum expected capacity of an associate for a given week. Variables include the maximum number of patients scheduled each hour and the number of patient contact hours.
Production Profile (Trend) – these variables help characterize the rate at which the associate will reach patient capacity. In other words, estimate how long will it take for their schedule to be full. In reality, it will never be a perfect line but it is only an estimate. This is controlled by specifying the number of patients per week for the first month and the increase in patients per week for each subsequent month. For example, in the first month, the associate sees 10 patients each week and in each subsequent month it increases by 5 so the production profile will look like 10 per week for month 1, 15 per week for month 2, 20 per week for month 3 and so on.
Compensation Simulation
Model the number of patients estimated per week and the rate at which weekly appointments increase until capacity is reached. Capacity is based on appointments scheduled per hour and hours per week.
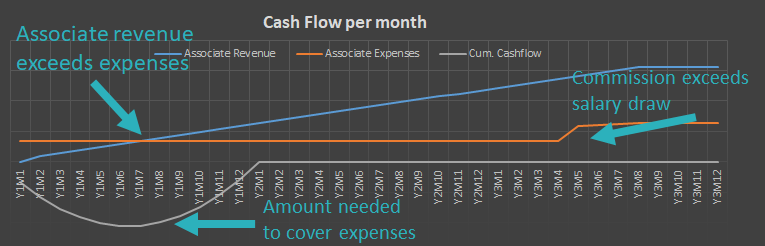
Calculate the revenue generated by the production profile. Consider expenses associated with hiring an associate. Determine the total financial risk or cash required to hire an associate before their production covers their expenses. Considering the compensation model, expenses increase when production exceeds the cumulative salary draw.

Based on a commission plus draw compensation model, estimate when the cumulated commission exceeds the cumulative draw. This is when the salary draw can be increased since the commission earned has exceeded the amount paid.
This analysis can be used to communicate to a potential associate “when” their compensation will increase based on the schedule trend. In the real world, these trends will not be “clean”. There will naturally be noise in the trendlines due to many factors including seasonal effects. It is important to overestimate your expenses and underestimate your revenue variables for a more conservative benchmark.
